
Pain, Maps, and Meaning: Part 1 - Reimagining Imaging
Jun 13, 2026
This is the first installment of a multi-part series.
An Image About Imaging
A few weeks ago, I came across an infographic I had first seen years ago. It summarized a number of imaging studies (links below) showing a high incidence of tissue abnormalities in asymptomatic subjects. For people in pain, findings like disc bulges, meniscal tears, rotator cuff tears, labral injuries, Morton’s neuroma, and spinal degeneration can be frightening and routinely trigger treatment plans, including surgery. Yet reputable studies have shown that these exact same findings also appear in surprisingly large numbers of people reporting no symptoms at all.
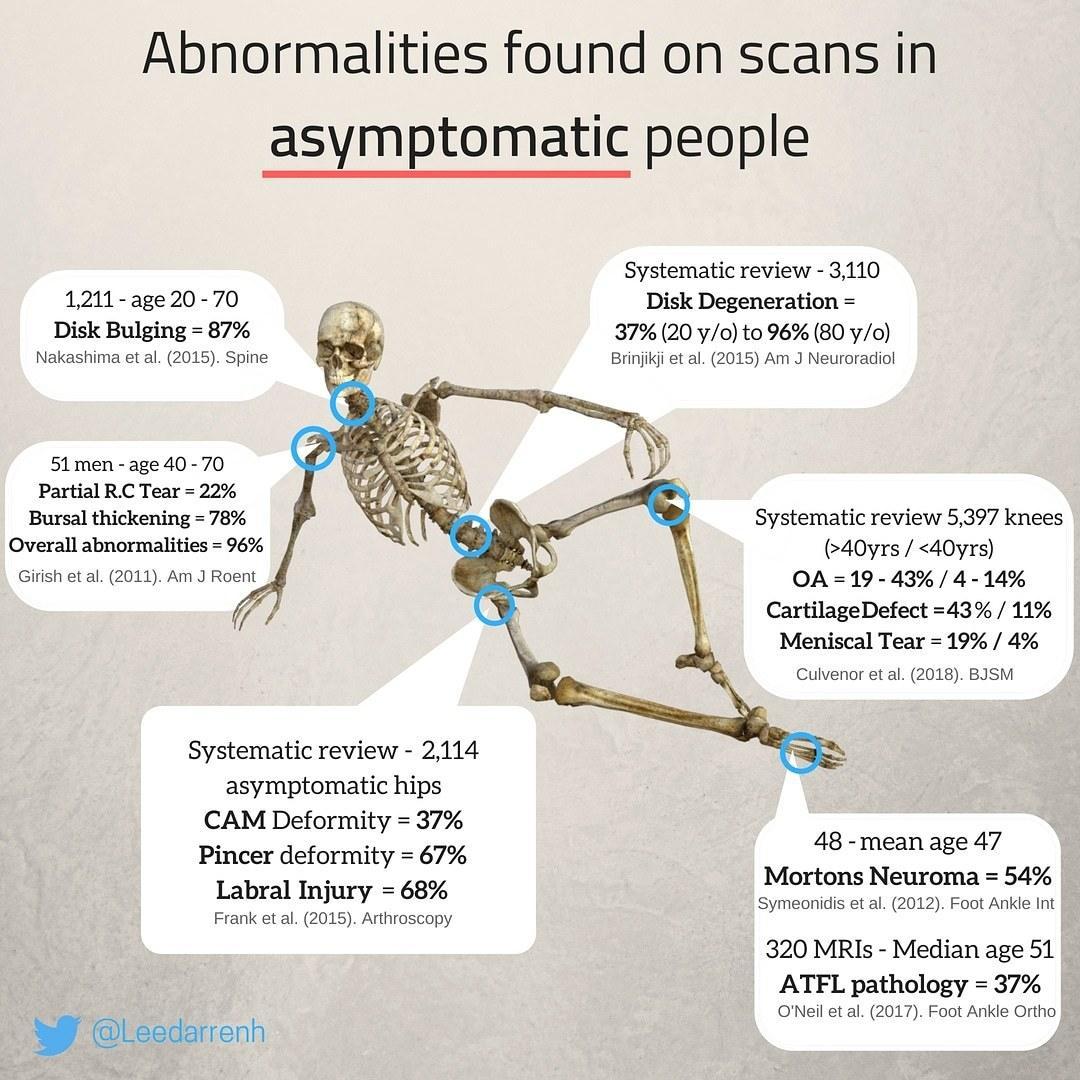 If I had to sum up the message of the chart, it would be something like this: the strongest correlation between pain and "abnormal" imaging findings may simply be that people in pain are the ones getting imaged.
If I had to sum up the message of the chart, it would be something like this: the strongest correlation between pain and "abnormal" imaging findings may simply be that people in pain are the ones getting imaged.
As we have all heard, correlation is not causation, and when it comes to living systems like human bodies, simple stories rarely explain why we suffer.
The Map vs. The Territory
My experience has taught me that medical imaging can reveal important information about tissue history, accumulated load, adaptation, and the ordinary consequences of inhabiting a body for decades in a gravity field. But even the most detailed MRI can only produce a limited map.
In the third edition of Yoga Anatomy, Amy Matthews and I referenced Alfred Korzybski’s famous observation that “the map is not the territory.” A map can be extraordinarily useful, but by definition it is highly selective. Maps highlight certain features while leaving others out, and an MRI works much the same way. It can reveal anatomical details with astonishing precision, but what it cannot reveal is the lived experience of the person standing inside that territory: how much pain they feel, how threatened they feel, how confidently they move, how they breathe, how they sleep, or how much fear and meaning become attached to an image-based diagnosis.
None of this means imaging is meaningless, nor should structural findings be dismissed out of hand. Acute injuries are real. Arthritis is real. Degeneration is real. Tissue matters. Inflammation matters. Yet when it comes to chronic pain, structure alone rarely explains enough, and these studies raise an uncomfortable question: if so many abnormalities coexist peacefully with ordinary function, what exactly are we seeing when we look at scans?
Structural Medicine Has Limits
To understand how we arrived here, it helps to appreciate why medicine became so structurally oriented in the first place. When someone fractures a bone, tears a ligament, develops an infection, or suffers acute trauma, tissue matters enormously. One of the reasons why modern medicine became so extraordinarily successful was because it learned how to identify physical problems and fix them. Once technologies like MRI allowed physicians to peer inside the body in exquisite detail, it was entirely reasonable to assume that once you can see more, you can also understand more.
Yet as imaging improved, clinicians began discovering something increasingly difficult to reconcile with a purely structural model: people with frightening scans were observed to be functioning remarkably well, while others with ordinary scans were clearly suffering terribly. Structure mattered, but the relationship between tissue and pain turned out to be far less predictable than many had assumed.
As a bodyworker, yoga educator, anatomy teacher, and occasional pain patient, these are questions I’ve been asking for decades. My own attempts to understand the relationship between structure and pain eventually led me to the work of the late John Sarno, M.D., whose ideas challenged many of the assumptions of rehabilitative medicine.
In the next installment of Pain, Maps, and Meaning, I will discuss the work of Dr. Sarno, as well as my points of agreement and disagreement with his theories. I will also discuss a post from several years back that tells the story of my own "Sarno moment" of debilitating back pain.
If you have received value from my writing, please consider supporting it by subscribing to my online community. You will gain access to my online courses, monthly Q&A Zoom chats, and hundreds of hours of educational content.
Here are links to the published studies referenced in the graphic above.
Nakashima et al. (2015), Spine
Abnormal Findings on MRI of the Cervical Spines in 1211 Asymptomatic Subjects
https://pubmed.ncbi.nlm.nih.gov/25584950/
Brinjikji et al. (2015), AJNR
Systematic Literature Review of Imaging Features of Spinal Degeneration in Asymptomatic Populations
https://pubmed.ncbi.nlm.nih.gov/25430861/
Girish et al. (2011), AJR
Ultrasound of the Shoulder: Asymptomatic Findings in Men
https://pubmed.ncbi.nlm.nih.gov/21940544/
Frank et al. (2015), Arthroscopy
Prevalence of Femoroacetabular Impingement Imaging Findings in Asymptomatic Volunteers: A Systematic Review
https://pubmed.ncbi.nlm.nih.gov/25636988/
Culvenor et al. (2018/2019), BJSM
Prevalence of knee osteoarthritis features on MRI in asymptomatic uninjured adults: a systematic review and meta-analysis
https://pubmed.ncbi.nlm.nih.gov/29886437/
Symeonidis et al. (2012), Foot & Ankle International
Prevalence of Interdigital Nerve Enlargements in an Asymptomatic Population
https://pubmed.ncbi.nlm.nih.gov/22835390/
O’Neil et al. (2017), Foot & Ankle Orthopaedics
Anterior Talofibular Ligament Abnormalities on Routine MRI Imaging of the Ankle
https://journals.sagepub.com/doi/10.1177/2473011417S000311
Stay connected with news and updates
Join our mailing list to receive news and updates from Leslie.
Don't worry, your information will not be shared.
We hate SPAM. We will never sell your information, for any reason.
